
Urostomy – Everything you need to know
In Germany itself, there are over 150,000 people with a stoma, many of them with an urostomy. After colon and intestinal stomas, urostomies are the third most common type of stoma. It is therefore important to understand what exactly a urostomy is and which surgical procedures are associated with it.
What is an urostomy?
The word stoma originally comes from the Greek and means ‘opening’. In general terms, a stoma is an artificially created connection between a hollow organ and the surface of the body.A urostomy is an artificial urinary diversion through the abdominal wall. It can or must be placed if the bladder or urinary tract is damaged or diseased and controlled urination is not possible. As a result, urine is constantly discharged as the urinary bladder is usually missing as a reservoir or is no longer functional. The urostomy itself refers to the actual surgical procedure to create an artificial urinary drainage system.
Basically, there are two different types of urostoma: continent and incontinent urostoma. Depending on the type, they channel urine constantly to the outside (incontinent urostoma) or collect it in a surgically created reservoir from where it can be emptied in a controlled manner (continent urostoma).
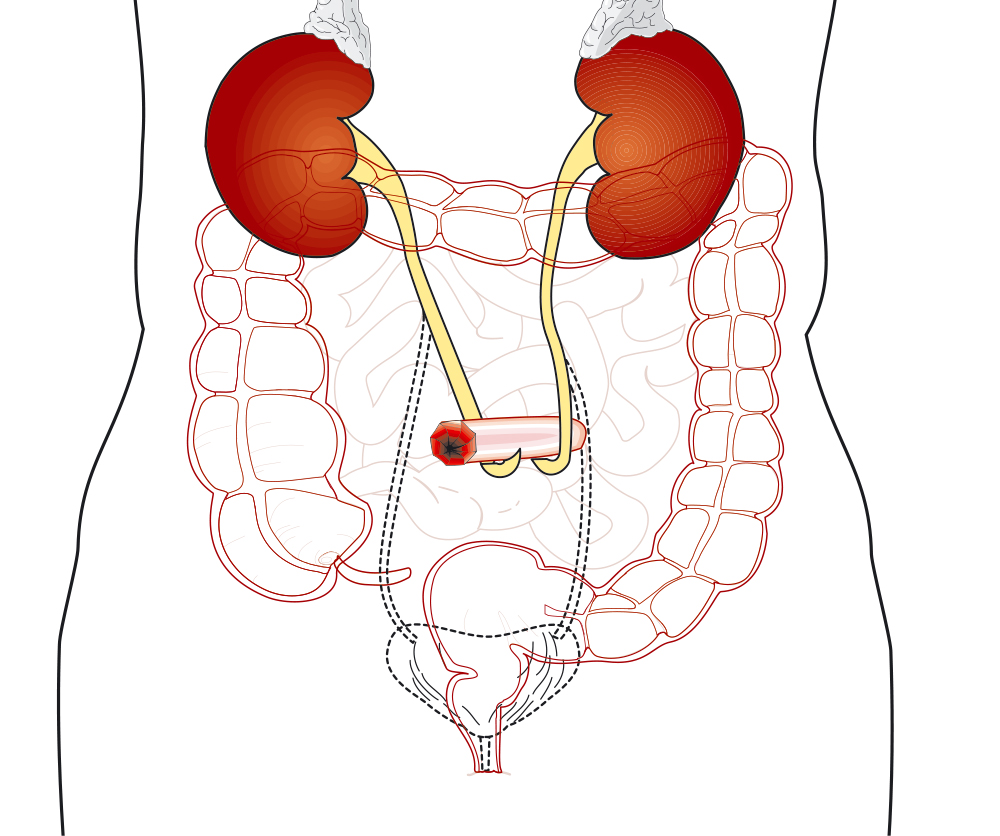
Essentials: The human urinary tract
The normal urinary tract comprises two kidneys, two ureters, a bladder and a urethra. Urine is produced in the kidneys and passes through both ureters to the bladder. The urine is then stored in the bladder until it is approximately half full. The urine is then discharged from the body through the urethra.A urostomy is therefore the creation of a new route for urine to pass through the stoma, out of the body and into a urostomy bag. This surgical route allows the urine to flow without any interference so that the kidneys can function at optimum efficiency.
Why is a urostomy required?
There are many reasons why a person might need a urostomy. These are due to a diseased bladder or a defect with the urinary system that needs to be bypassed. Social reasons are also often cited for the decision to have a urostomy. As those affected with a defective bladder are often unable to control their urine flow, this completely restricts their life - both privately and at work. The following are a few typical reasons that may require a urostomy:- Diseased bladder, for example due to cancer
- Birth defects such as spina bifida that affect the urinary tract
- Diseases such as multiple sclerosis, cerebral palsy and spinal cord injuries can cause nerve damage that leads to bladder dysfunction
- Gynaecological problems, urinary fistula or other conditions in which the bladder or sphincter muscles do not function properly
- Chronic inflammation: painful bladder syndrome or interstitial cystitis
- Trauma or injury of the bladder
What happens during a urostomy operation?
As there are different types of surgery, all options will be discussed in detail with your surgeon before your operation. Which type of urinary drainage is most suitable for you depends on various factors. Diagnosis, age, medical history, previous operations, how well you can move and whether you have good dexterity in your hands are all taken into account when making this decision.Incontinent urinary drainage
Incontinent urinary drainage refers to an artificial bladder outlet in which urine is continuously drained from the bladder via a stoma into a stoma pouch. It is therefore not possible to drain the urine in a controlled manner.Ileum-Conduit
The most common operation for urinary drainage after complete removal of the bladder is the ileum conduit.The surgeon uses a section of the small intestine (ileum) about 12-14 cm long to form the ileum conduit. The remaining intestine is then reconnected and can therefore function normally. The ureters are then separated from the bladder and sewn into the conduit, which is attached to the abdominal wall to create a stoma. This allows urine to pass directly from the kidneys to the outside via the ureters. As there are no muscles to control urine excretion, a urostomy pouch is required. This pouch covers your new stoma and adheres to your abdomen.
Nice to know: During the operation, fine tubes, so-called "stents", are inserted into the kidneys via the ureters. These support the free emptying of urine until healing is complete. These stents either fall out on their own or are removed around 10 days after the surgery. Your stoma nurse will monitor this as soon as you are back home.
Ureteral fistula
In the case of a ureteral fistula, the ureter is channelled to the outside through the abdominal wall. Depending on the clinical symptoms, this can work independently for one kidney (Transureterocutaneostomy or TUC) or for both kidneys (Transureteroureterocutaneostomy or TUUC). The ureters can therefore be drained on one or both sides.Continent urinary drainage
Continent urinary drainage, such as the creation of a neobladder or a Mitrofanoff reservoir, is considered a urinary reconstruction and is an alternative to ileum conduit surgery. In order to be able to undergo these two operations, the risk of cancer recurrence must be low. Immediately after the operation, you will learn how to catheterise yourself, as this is necessary in the long term to drain the urine. Manual dexterity is definitely an advantage here.Please note that a certain amount of urinary incontinence (dribbling) is completely normal in the first 6 months and therefore it is useful to wear a sanitary pad.
Neobladder
A neobladder is a surgically formed, artificial urinary bladder. It is used as a replacement after a cystectomy (bladder removal) and is one of the continent urinary drainages.During a neobladder procedure, your surgeon uses a larger section of your bowel to create something like a replacement bladder. This will be connected to the urethra. In this way, you can pass urine normally, but you no longer have the normal muscle reflexes that control the emptying of the bladder. It is therefore quite possible that you will have to catheterise yourself in order to empty the bladder completely.
Mitrofanoff-Reservoir
The Mitrofanoff stoma is also a continent stoma. In order to gain access to the bladder, the appendix is sewn in as a canal between the abdominal wall and the bladder. Urine is regularly drained from the bladder via the stoma using a catheter.After urostomy surgery
It is perfectly normal to feel very tired in the weeks following the procedure. Be gentle with yourself and your body. Always remember that such a major operation is incredibly stressful and your body needs time to heal and adapt. Don't rush things in the first 6 to 8 weeks and take the time to recharge your batteries. Nevertheless, it is important to stay mobile. Each following week you will realise that you can manage a little more. However, try not to bend down or lift heavy objects. This could impair your regeneration.It takes about 8 to 12 weeks to fully recover from stoma surgery. You can find more detailed information about recovery after a stoma operation here.
Stoma care
The stoma itself is red in colour and feels moist. In a normal environment, the bowel produces mucus to support lubrication - it continues to do this even after the stoma has been created. You will therefore notice white, jelly-like mucus on your stoma in the first few weeks. The amount varies from person to person, but should slowly decrease over time.The stoma has no sensory nerve endings and is therefore completely non-irritating. It therefore does not cause any pain if touched, but can be somewhat sensitive at the edges at first. The stoma is very well supplied with blood and can bleed easily during cleaning. A few blood stains while cleaning the stoma are nothing to worry about. Nevertheless, handle your stoma with caution.
Tips & Tricks:
- Wash your stoma and the surrounding skin with warm water before applying a new stoma pouch.
- Try to avoid soaps or perfumed sanitary products.
- Take enough time to check your stoma and the surrounding skin to ensure there is no irritation.
- Gently pat the skin and the stoma dry before applying a new pouch.
Your stoma will slowly reduce its shape and size in the first 6 to 8 weeks after the surgery. It is therefore quite possible that you will need to adjust your appliance to match your stoma's new size. Your stoma care nurse will help you to determine the correct size of your stoma and find the optimal appliance for you.
More about ostomy care:
- My stoma, my skin and me – Feeling good starts with the right care
- Showering & bathing with a stoma – turning your skincare routine into a feel-good experience
Emptying and changing the pouch
Empty the pouch regularly, preferably as soon as it is one third to half full. A urostomy pouch stores the same amount of urine as your bladder. You therefore only need to empty it as often as you urinated before your operation.
In general, change the pouch every day or every two days. This depends on how well the pouch adheres to your skin, whether you have any leakages and how active you are. A skin protectin ring can provide you additional security and extends the wearing time of your pouch.
There are also drainage bed bags that continuously drain the urine from the urostomy pouch and enable you to avoid emptying the pouch overnight. However, such pouches are a personal preference and are not essential.
You can find out more about this topic here.
Sexuality
Depending on the scope of the surgery, it is not unusual to experience physical changes in sexual function. Your surgeon will inform you of this risk before your procedure. Nerve damage can affect both men and women.
Basically, you should be patient with each other. Intimacy with a stoma is still possible as normal. However, insecurities about how your body feels are just as normal too. So approach the situation sensitively, talk about your feelings and please don't put yourself under pressure. If you have any difficulties regarding this, speak to your trusted stoma care nurse. He or she will be able to give you advice and support.
Urostomy care
There are many different types of urostomy pouches. Your stoma care nurse will help you choose one that feels comfortable and is aesthetically pleasing. All pouches are usually waterproof, odour-proof and have a well-proven skin protection that works as a barrier for your skin. Urostomy pouches have a non-return valve that prevents urine from running back over the stoma. In addition, the pouches all have an easy-to-use closure that allows the urine to be drained easily into the toilet.
Discover our extensive portfolio of urostomy products here.
 For more information about us or our products, please visit our website. There you will find, among other things, our detailed FAQ and other interesting blog articles all about the topic stoma. You can also contact us via our social media channels or send us an e-mail. We look forward to hearing from you!
For more information about us or our products, please visit our website. There you will find, among other things, our detailed FAQ and other interesting blog articles all about the topic stoma. You can also contact us via our social media channels or send us an e-mail. We look forward to hearing from you!
The contents of this blog, including all text, graphics, images and information, are intended for informational purposes only. They are not a substitute for professional medical advice, diagnosis or treatment. Always consult a qualified healthcare professional if you have any questions about a medical condition or treatment, and before starting any new healthcare treatment. Reliance on any information provided on this website regarding health related decisions are solely at the reader's own risk.